Solid phase extraction (SPE)
Published over 10 years ago. See the latest and most current information on Solid phase extraction (SPE).
Although urine testing has become routine in laboratories tasked with finding evidence for consumption of marijuana or other cannabis containing products, oral fluid is emerging as an attractive alternative due to its non-invasive sampling procedures. However, because drug and metabolite levels are very low in oral fluid, a very sensitive analytical method is required. In this article, we describe a new sample preparation procedure using micro-elution SPE that reduces the time and effort required to generate samples for LC-MS/MS analysis of THCA from both urine and oral fluid. The LC-MS/MS method has a Limit of Quantification (LOQ) for THCA below 1.5 ng/mL in urine and 10 pg/mL in oral fluid.
Marijuana is one of the most commonly consumed drugs due to its psychoactive effects, and is therefore frequently found in forensic and toxicology analyses [1]. Although its use has been illegal for some time, marijuana and other forms of cannabis are being accepted around the world including some parts of the United States for medicinal and recreational use. Because of this widespread use, laboratories have a pressing need to rapidly and reliably analyse samples to detect marijuana and cannabis consumption.
THC ((-)-Δ9-Tetrahydrocannibinol) is the primary psychoactive component in marijuana and cannabis products. In the body, THC is metabolised to form THC-OH ((±)-11-Hydroxy-Δ9-Tetrahydrocannibinol), which is also psychoactive, and THCA ((±)-11-nor-9-Carboxy-Δ9-Tetrahydrocannibinol), which is not. These metabolites persist for days following consumption, enabling their use as markers for recent cannabis use [2]. Blood can contain all three components, while urine typically contains only THCA. Oral fluid can contain both THC and THCA. However, it is possible for THC to collect in oral fluid from passive exposure in environments where marijuana is being smoked, and so THCA detection is therefore required to conclusively identify cannabis consumption from oral fluid samples.
Chromatographic methods for the detection and quantification of these compounds were originally developed based on GC-MS [3-4], however this approach requires extensive sample preparation and derivatisation prior to analysis. More recently, LC-MS/MS has become more widely available and accepted for these analyses, providing simplified workflows through the elimination of the derivatisation step [5-6]. LC-MS/MS also allows flexibility by enabling concurrent analysis for other drugs, extending the range of a single test.
Sample preparation plays a major role in any analysis involving biological fluids or tissues since there are many components in these matrices that are either incompatible with the analytical system or produce interferences with the target compounds. For example, blood contains a high concentration of proteins and phospholipids that can foul the analytical column and result in ion suppression during MS detection. Urine contains a high salt concentration that can precipitate throughout the system, especially at the ion source, necessitating frequent maintenance.
Different approaches have been described for the extraction of THC and its metabolites from urine and oral fluid, mostly involving Liquid-Liquid Extraction (LLE) [7] or Solid Phase Extraction (SPE) [8-9]. Although these techniques are efficient at removing matrix components that negatively impact the analysis, they have extensive time and solvent requirements, and the multiple steps can lead to the introduction of error and imprecision.
Micro-elution SPE is based on smaller media bed weights (2 mg) than are typically used for SPE. Although the smaller beds have lower loading capacities than larger beds, methods based on micro-elution SPE benefit from using less solvent during elution. This reduces the amount of time required for evaporation prior to reconstitution for analysis, or can eliminate this process completely, which has significant advantages to reducing non-specific binding which can have adverse effects on the recovery, particularly of larger molecules.
In this article, novel sample preparation approaches are presented for the analysis of THCA in urine as well as the analysis of THC and THCA in oral fluid that enables reliable detection and quantification of THCA at the low levels required for using this matrix to positively identify cannabis usage. Sample preparation is based on micro-elution solid phase extraction using a polymeric mixed-mode (reversed phase/strong anion exchange) sorbent, enabling the use of small sample and elution volumes to facilitate LC-MS/MS analysis without the need for evaporation and reconstitution of the extract. Mass spectral detection was performed using a triple stage quadrupole mass spectrometer in SRM mode.
THC, THC-d3, THCA, and THCA-d3 were purchased as solutions in MeOH from Cerilliant Corporation (Round Rock, TX). LC-MS Optima Grade Water and Acetonitrile, and LC/MS Grade Formic Acid were purchased from Fisher Scientific (Waltham, MA) and used as supplied. Human urine and oral fluid samples were obtained from volunteers and was tested to ensure that it was free of THC and THCA prior to use.
Separations were performed using a Thermo Scientific™ UltiMate™ 3000 RSLC system coupled to either a Thermo Scientific™ TSQ Endura™ (urine) or Thermo Scientific™ TSQ Quantiva™ (oral fluid) triple stage quadruple mass spectrometer, each equipped with a heated electro spray ionisation source, HESI II.
Solid phase extraction using Thermo Scientific™ SOLAµ™ SAX (2 mg/1 mL, 96-well plate) was utilised for both urine and oral fluid samples. Although different sample pretreatment procedures were utilised for the two matrices, the SPE procedures were the same. The full sample preparation procedure is summarised in Figure 1.
Urine was treated through base hydrolysis with concentrated NaOH prior to solid phase extraction to convert THCA-Glucuronide to its native form to simplify data analysis and interpretation. Silanised vials were used for the hydrolysis to reduce binding of THCA to the vials walls during the process. To 100 µL of urine, 10 µL of internal standard (THCA-d3, 150 ng/mL in ACN) and 20 µL 9M NaOH were added, and the sample was incubated at 60°C for 20 minutes. Once cool, the sample was diluted with 200 µL ACN and neutralised with 10 µL glacial acetic acid. Final dilution with 200 µL 20 mM NH4OAc was performed to prepare the sample for the solid phase extraction procedure.
Oral fluid was treated through mild protein precipitation prior to extraction. A combination or oral fluid and preservation buffer (750 µL total volume containing 250 µL of oral fluid) was treated with 200 µL ACN and 25 µL of internal standard solution (THCA-d3 at 1 ng/mL and THC-d3 at 10 ng/mL), followed by 50 µL of 1% NH4OH solution.
Treated samples were then loaded into the SOLAµ SAX well plate and drawn through under vacuum. Samples were washed with 200 µL of H2O/ACN (50:50 v:v) before elution with ACN/Formic Acid (95:5 v:v) into Thermo Scientifc™ WebSeal™ Glass Inserted plates. Urine samples were eluted with two 50 µL aliquots, while oral fluid samples were eluted with two 30 µL aliquots. Extracts were diluted 1:1 with H2O prior to injection.
LC separations were performed using Thermo Scientific™ Accucore™ RP-MS analytical column (100 x 2.1 mm, 2.6 µm) with Mobile Phase A containing 0.1% formic acid in water and Mobile Phase B containing 0.1% formic acid in acetonitrile at a flow rate of 0.40 mL/min. An initial mobile phase composition of 60% B was held for 0.50 minutes before applying a linear gradient to 95% B for 3.0 minutes before a hold time of 0.50 minutes. The mobile phase was returned to the initial conditions for column equilibration, resulting in a total run time of 5.0 minutes. Mass data was acquired in SRM mode using the ion source conditions and MS/MS transitions listed in Table 1.
When determining the amount of THCA in urine, samples should be hydrolysed with strong base to convert any THCA-glucuronide present into the uncomplexed form to simplify the analysis and data interpretation. Although it is possible to inject the hydrolysed samples following neutralisation and dilution, this introduces contaminants and potential interferences that can negatively impact the lifetime of the analytical column and the overall cleanliness and hence sensitivity, of the mass spectrometer. Solid phase extraction is an alternative that produces much cleaner samples. However, any method involving solid phase extraction should be as simple as possible to facilitate rapid sample preparation and reduce the potential for errors.
The procedure developed here involves base hydrolysis with concentrated NaOH followed by dilution and neutralisation. Analytes are then extracted from the hydrolysed sample followed by micro-elution solid phase extraction using a mixed-mode (reversed-phase/strong anion exchange) sorbent. This kind of material provides high selectivity for acidic analytes, resulting in cleaner extracts that eliminate more contaminants and interferences to produce better analytical column lifetimes and reduces intervals between instrument maintenance. Elution is performed using acetonitrile with 5% formic acid, generating a sample that can be injected into the LC-MS/MS system following dilution with water, eliminating the common evaporation and reconstitution steps while still meeting necessary detection limits.
Guidelines provided by the Substance Abuse and Mental Health Services Administration (SAMHSA) set a cutoff for a positive THCA determination in urine is 15 ng/mL [10]. To ensure that the method would meet requirements by having a limit of detection at or below 10% of the cutoff value, linearity was determined by spiking blank urine with THCA in concentrations from 0 to 100 ng/mL. The ratio of the peak area for THCA to the peak area for the internal standard (THCA-d3) was used to calculate the response for each sample. Linear response over the full range was observed with no weighting (R2=0.9992) (Figure 2a) with the lowest concentration standard (1.5 ng/mL) showing more than adequate signal-to-noise (Figure 2b). Although a true limit of detection was not determined for the method, this result suggests that it is well below the 10% of cutoff threshold.
Recovery of THCA from the solid phase extraction process was assessed by comparing the THCA peak area for samples spiked with THCA before and after extraction for three different concentrations (1.5, 15, and 40 ng/mL). Six replicates were performed at each concentration level. At all three levels, recoveries greater than 92% were observed for THCA with high reproducibility indicated by %RSD less than 5.4%. Minimal matrix effects were observed by comparing post-extract spiked samples to samples prepared by spiking the same amount of THCA into the elution solvent.
Quality control samples were prepared by spiking blank urine with THCA at concentrations above and below the cutoff limit. These samples were extracted and analysed, and the calculated concentrations were compared to the actual concentrations. Six replicates were analysed at each concentration. For all samples, the calculated THCA concentration agreed with the actual concentration to within 5%.
Oral fluid is a challenging matrix to work with due to the generally lower concentrations of drugs and metabolites relative to other fluids such as urine and blood [11]. For example, while analytical methods for determining THCA levels in urine need only to be suitable to concentrations around 1.5 ng/mL, methods for determining THCA in oral fluid must be capable of detecting and quantifying at levels of around 10 pg/mL [12].
A variation on the sample preparation procedure described above for urine has been applied to oral fluid. Sample pre-treatment has been modified to be more appropriate to the different matrix, using dilution with acetonitrile to help with protein removal and solubilisation of THCA. Again, while it is possible to analyse oral fluid following simple dilution, solid phase extraction is generally a better approach since the sample can be concentrated down through the extraction procedure. A similar solid phase extraction procedure using SOLAµ SAX with a mixed-mode reversed-phase/strong anion exchange sorbent was used, with elution using acetonitrile with 5% formic acid that can be diluted with water prior to injection.
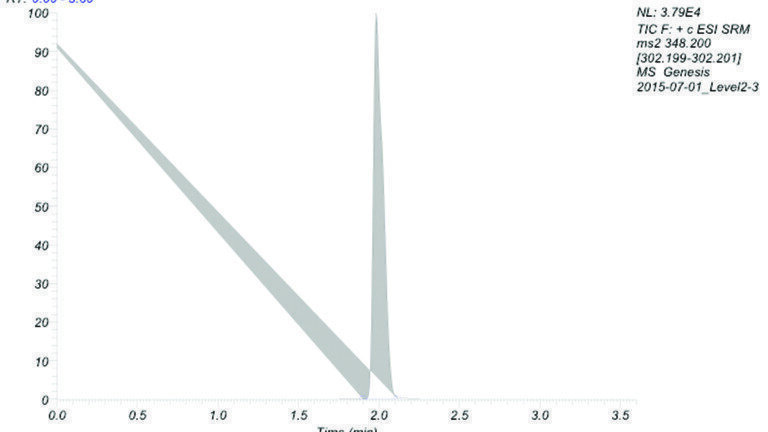
Limits of quantification (LOQs) were defined as the lowest concentrations that had back-calculated values within 20%, and RSD for five QC replicates within 20%. Using these criteria, the limit of quantitation was 10 pg/mL for THCA and 0.5 ng/mL for THC in oral fluid. Linearity was determined from 0 to 1000 pg/mL for THCA and 0 to 1000 ng/mL for THC. Calibration curves and chromatograms of the lowest standard are shown in Figure 3a,b for THCA and Figure 4a,b for THC, and both compounds displayed linear response over the concentration range.
Recovery was determined by spiking 50 pg/mL of THCA and 5 ng/mL THC into five donor samples before and after SPE. These samples showed an average recovery of 98.1% for THCA and 61.6% for THC.
Samples for determining the precision of the sample preparation and analytical procedure were prepared by spiking oral fluid with THCA and THC at three different concentration levels (25, 100, and 500 pg/mL for THCA and 2.5, 10, and 50 pg/mL for THC). Four replicates were analysed in three separate batches. The %RSD across these samples was less than 8.5% for THCA and less than 3.2% for THC for all three concentration levels (Table 2), indicating the reliability of the method to produce precise analyte concentrations.
In this report, we have demonstrated a sample preparation method for urine and oral fluid based on micro-elution SPE. This method enables rapid analyte extraction from the sample with high recoveries and precision. More importantly, the method requires fewer steps and less time than method using conventional SPE formats. Extracts can be analysed without evaporation and reconstitution prior to LC-MS/MS analysis, instead only requiring dilution. This approach has been demonstrated to be suitable for achieving the very low detection limits required for analysing THCA in oral fluid.
[1] United Nations Office on Drugs and Crime. World Drug Report (2013).
[2] R. Baselt. Disposition of Toxic Drugs and Chemicals in Man, 8th Edition. Atlas Books, Ashland, OH, 2008.
[3] B.D. Paul, L.D. Mell, Jr., J.M. Mitchell, and R.M. McKinley. J. Anal. Toxicol. 11 (1987) 1.
[4] P. Kintz, V. Crimele. Biomed. Chrom. 11 (1987) 371.
[5] B. Maralikova and W. Weinmann. J. Mass Spectrom. 39 (2004) 526.
[6] F.T. Peters. Clin. Biochem. 44 (2011) 54.
[7] M.H. Chu and O.H. Drummer J. Anal. Toxicol. 26 (2002) 575.
[8] R.A. Gustafson, E.T. Moolchan, A. Barnes, B. Levine, M.A. Huestis. J. Chromatogr. B Analyt. Technol. Biomed. Life Sci. 798 (2003) 145.
[9] J.L. Schroeder, L.J. Marinetti, R.K. Smith, W.E. Brewer, B.L. Clelland, and S.L. Morgan. J. Anal. Toxicol. 32 (2008) 659.
[10] Federal Register, 73 FR 71858, Section 3.4, 2008.
[11] M.A. Huestis, A. Verstraete, T.C. Kwong, J. Morland, M.J. Vincent, R. De La Torre. Clin Chem. 57 (2011) 805.
[12] D. Lee, G. Milman, A.J. Barnes, R.S. Goodwin, J. Hirvonen, M.A. Huestis. Clin Chem. 57 (2011) 1127.